Investigating and Exploring the Neuroprotective Effect of Metformin, Vitamin E and Co Enzyme Q10 in Neonatal Rat Model of Hypoxic-Ischemic Encephalopathy
Volume 1, Issue 1, Pages 1-9
History
Received 10 November 2025
Revised 26 November 2025
Accepted 03 December 2025
Keywords
Neonatal hypoxic-ischemic encephalopathy, Oxidative stress, Vitamin E, Coenzyme Q10, Neuroprotection, Antioxidants, Synergistic therapy, Metformin.
Open Access
This is an open access article under the CC BY license https://creativecommons.org/licenses/by/4.0/.
Funding
BIOCHEMICAL ASSAYS
Effect of Treatment Drug on Oxidative Stress Markers
Challenging the animals with HIE followed by treatment with hypothermia significantly caused oxidative damage (Table 4) as indicated by increased in lipid peroxidation (MDA level), it caused by oxidative damage significant in brain cortex of HYPO group while decreased superoxide dismutase (SOD), and glutathione (GSH) activity in whole brain region. Pre-treatment with MET (200 mg/kg), Vit E (100 mg/kg) and CoQ10 (200 mg/kg) significantly restored depleted GSH (glutathione) and catalase activity as well as attenuated elevated lipid peroxidation of the brain, as compared to their respective control and HYPO group (Figures 1–3).
| Groups | SOD (IU/mg TP) | GSH (µg/mg TP) | LPO (µM/mg TP) |
|---|---|---|---|
| SHAM | 13.04 ± 0.32 | 83.20 ± 1.49 | 6.16 ± 0.47 |
| HIE + Hypothermia [HYPO] | 3.71 ± 0.07 a | 11.05 ± 0.48 a | 15.24 ± 0.61 a |
| HIE + Hypothermia + MET + Vit E | 9.10 ± 0.60 | 24.68 ± 2.91 a | 8.76 ± 0.29 a b |
| HIE + Hypothermia + MET + CoQ10 | 9.07 ± 2.40 | 21.96 ± 4.02 a | 8.15 ± 0.07 b |
| HIE + Hypothermia + MET + Vit E + CoQ10 | 11.56 ± 0.88 b | 69.73 ± 5.06bcd | 8.70 ± 0.58 a b |
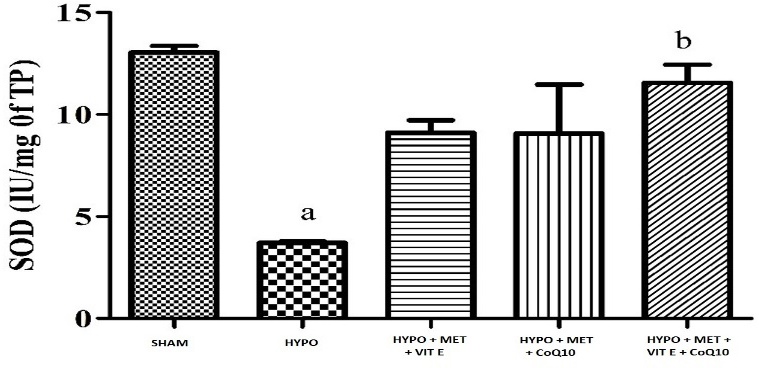
Figure 1 - Graph depicting SOD level in the brain. All data were expressed as Mean ± SEM. Statistical difference were determined by One-way ANOVA followed be Bonferroni’s Multiple Comparison test. Where the values are expressed as Mean ± SEM (n = 4). Where ap < 0.05 vs SHAM, bp < 0.05 vs HYPO, cp < 0.05 vs MET + Vit E and dp < 0.05 vs MET + Vit E + CoQ10.
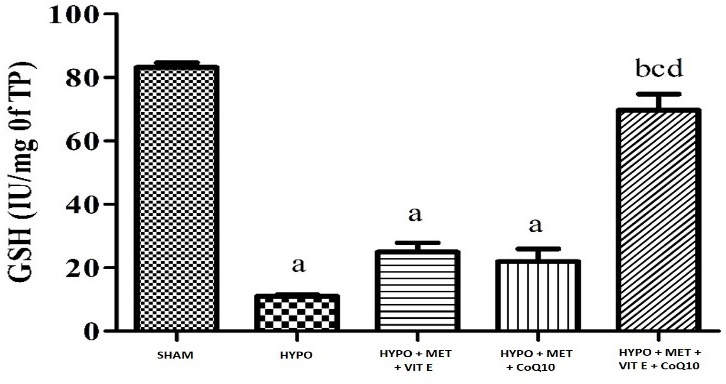
Figure 2 - Graph depicting GSH level in the brain. All data were expressed as Mean ± SEM. Statistical difference were determined by One-way ANOVA followed be Bonferroni’s Multiple Comparison test. Where the values are expressed as Mean ± SEM (n = 4). Where ap < 0.05 vs SHAM, bp < 0.05 vs HYPO, cp < 0.05 vs MET + Vit E and dp < 0.05 vs MET + Vit E + CoQ10.
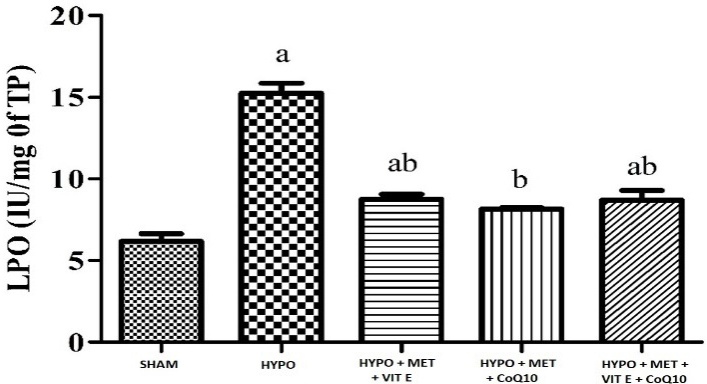
Figure 3 - Graph depicting LPO level in the brain. All data were expressed as Mean ± SEM. Statistical difference were determined by One-way ANOVA followed be Bonferroni’s Multiple Comparison test. Where the values are expressed as Mean ± SEM (n = 4). Where ap < 0.05 vs SHAM, bp < 0.05 vs HYPO, cp < 0.05 vs MET + Vit E and dp < 0.05 vs MET + Vit E + CoQ10.
TTC Staining for Infarct Volume
Ischemia injury causes infraction in the brain regions. In the HYPO group show severe cerebral infarction due to extensive damage inflicted by HYPO injury as compared with SHAM group. Pre-treatment with MET, Vit E and CoQ10 showed significant reduction in infarct area as compared with HYPO group. Whereas pre-treatment with MET + Vit E + CoQ10 along with hypothermia showed significant reduction in infarct area as compared with HYPO and MET, Vit E and CoQ10 treated group (Table 6, Figure 4).
| Groups | % Brain infarct area |
|---|---|
| SHAM | 6.11 ± 1.36 |
| HIE + Hypothermia [HYPO] | 44.11 ± 0.76 a |
| HIE + Hypothermia + Met + Vit E | 25.07 ± 1.37 a b |
| HIE + Hypothermia + Met + CoQ10 | 11.00 ± 0.63abc |
| HIE + Hypothermia + Met + Vit E + CoQ10 | 5.64 ± 0.21bcd |
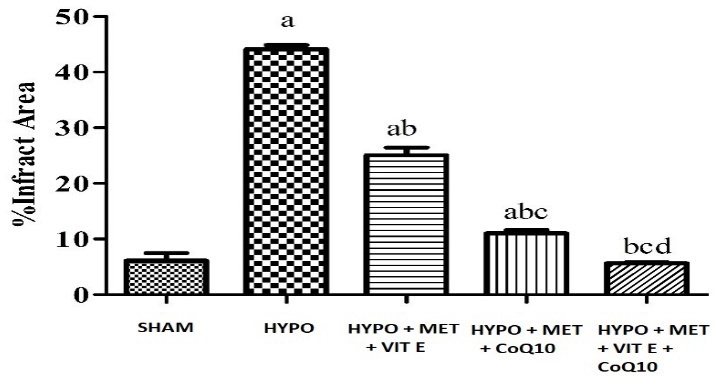
Figure 4 - Graph depicting % brain infarct area All data were expressed as Mean ± SEM. Statistical difference was determined by One-way ANOVA followed be Bonferroni’s Multiple Comparison test. The values are expressed as Mean ± SEM (n = 4). Where ap < 0.05 vs SHAM, bp < 0.05 vs HYPO, cp < 0.05 vs HYPO + MET + Vit E and dp < 0.05 vs HYPO + MET + CoQ10.
Infarct analysis (Coronal brain sections 2 mm), stained with 2% TTC, showing stained brain slices infarct area after 15 min bilateral common carotid artery occlusions followed by 24 h reperfusion in SHAM, HYPO and treatment groups pups (Figure 5). The red area represents the non-ischemic (viable tissue) area (Figure 6), whereas the white area indicates ischemic area (non-viable tissue) in the coronal section.
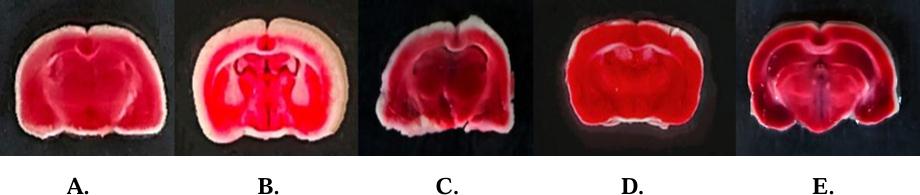
Figure 5 - Effect of MET, Vit E and CoQ10 on brain infarction Where A: SHAM; B: HYPO; C: HYPO + MET + Vit E; D: HYPO + MET + CoQ10; E: HYPO + MET + Vit E + CoQ10.
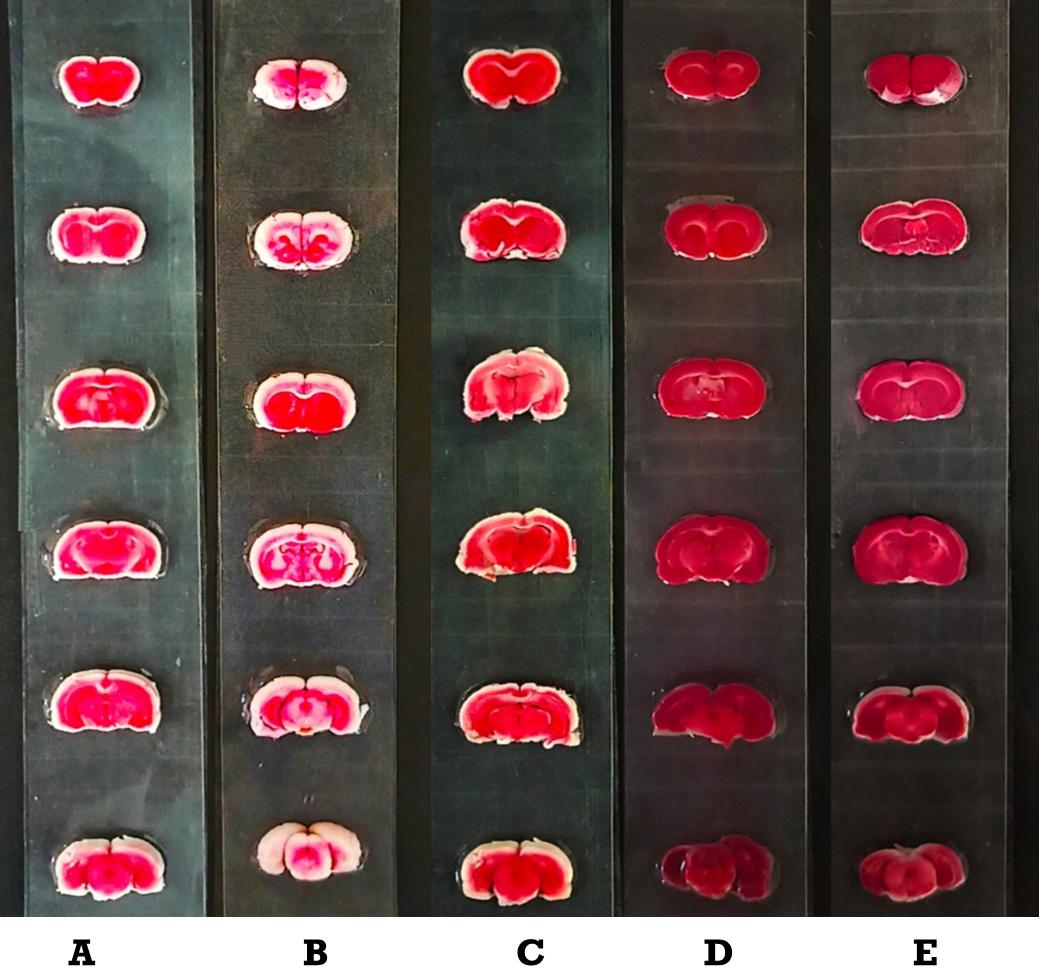
Figure 6 - Cerebral infarction. A: SHAM; B: HYPO; C: HYPO + MET + Vit E; D: HYPO + MET + CoQ 10; E: HYPO + MET + Vit E + CoQ10.
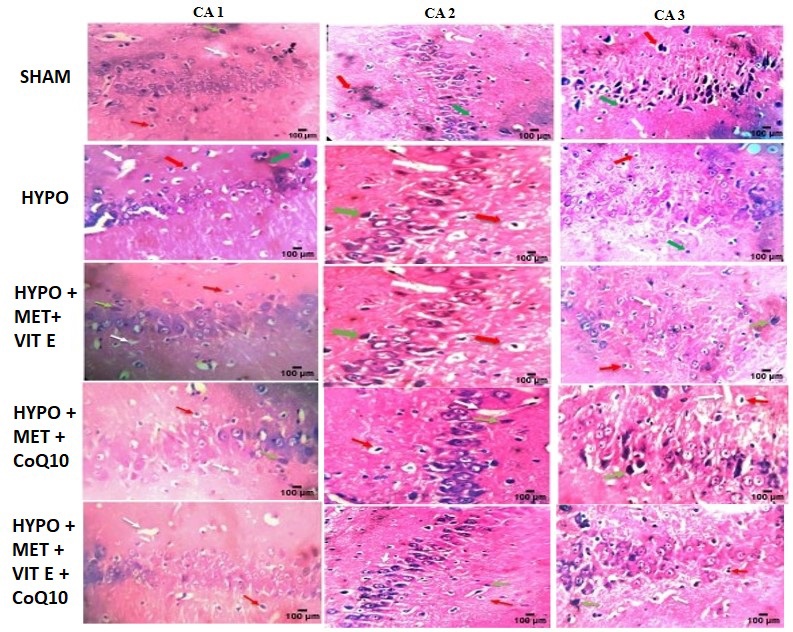
Figure 7 - Histopathology of brain.
Conflict of Interest
None to declare.
Author’s Contribution
Deepa Iyer and Rita Mourya designed the model and analyzed the data; Rajat Singh Rathore carried out the experiments and data collection; Naveen Gupta supervised the project and provided direction. All four authors have contributed significantly to the research conception and design, interpretation of data, and critical revision of the manuscript.